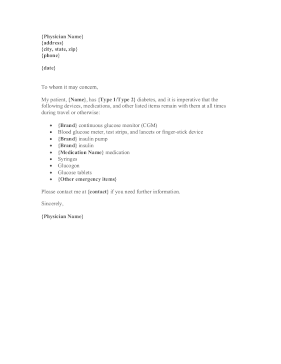
A person with Type 1 or Type 2 diabetes will find this letter from a doctor or endocrinologist helpful in explaining that glucose monitors, insulin pumps, lancets and other supplies must be carried on a plane, at school, and other times.

{Physician Name}
{address}
{city, state, zip}
{phone}
{date}
To whom it may concern,
My patient {Name} has {Type 1/Type 2} diabetes and it is imperative that the following devices, medications, and other listed items remain with them at all times during travel or otherwise.
{Brand} continuous glucose monitor (CGM)
Blood glucose meter, test strips, and lancets or finger-stick device
{Brand} insulin pump
{Brand} insulin
{Medication Name} medication
Syringes
Glucogon
Glucose tablets
{other emergency items}
Please contact me at {contact} if you need further
information.
Sincerely,
{Physician Name}